Acute otitis media in children | etiology, clinical features and Management
Definition
Acute suppurative otitis media (ASOM or AOM) is an acute inflammation of the middle ear.
Half of the cases occur in children younger than 5 years of age. After the introduction of the pneumococcal conjugate vaccine, the incidence of disease and its complication has reduced significantly especially in below 2 years of age-group.
Etiology
Bacterial
Pre pneumococcal vaccine era
- Streptococcus pneumoniae,
- Nontypable Haemophilus influenza
- Moraxella catarrhalis.
Post conjugate pneumococcal vaccine era
Nontypable H. influenzae (40-50% of cases )
Other
- Group A streptococcus,
- Staphylococcus aureus, and
- gram-negative organisms.
Viral
Viruses impair local immune function, inflammation of the eustachian tube, and increase bacterial adherence/colonization.
- Respiratory syncytial virus,
- rhinovirus,
- influenza viruses, and
- adenoviruses
Pathogenesis
Anatomical factors - Eustachian tube obstruction
Interruption of ventilation to middle ear mucosa by tubal obstruction initiates an inflammatory response that compromises the mucociliary transport system and causes effusion of liquid into the tympanic cavity.
- Extraluminal blockage by hypertrophied nasopharyngeal adenoid tissue or tumor.
- Intraluminal obstruction via inflammatory edema of the tubal mucosa.
- An excessively patulous or compliant eustachian tube may fail to protect the middle ear from reflux of infective nasopharyngeal secretions.
- Impairment of the mucociliary clearance leads to the establishment and persistence of infection.
- The shorter and more horizontal orientation of the tube in infants and young children increases the risk of reflux from the nasopharynx.
Host factors
- Acquired immunodeficiency such as HIV
- Congenital immunodeficiency such as Ig A deficiency and IgG sub-class deficiency.
Why is ASOM common in children?
- Eustachian tubes are shorter,
- More horizontal and
- More prone to obstruction by enlarged adenoids
- Predisposing factors like Viral infections and allergies are common in children
Clinical features
Symptoms
- Repeatedly rubbing, or holding the ear.
- Pain in ear
- Fever
- Irritability in younger children
- Lathargy
- Symptoms of upper respiratory tract infection like dry cough or rhinorrhea
Signs

|
| Structure of Normal tympanic membrane - source 1 |
- Middle ear effusion
- Signs of middle ear inflammation on otoscopic examination
- Moderate to severe tympanic membrane (TM) bulging
- Mild bulging of the TM associated with recent onset of otalgia less than 48 hours or erythema.
- Otorrhea that is not caused by otitis externa
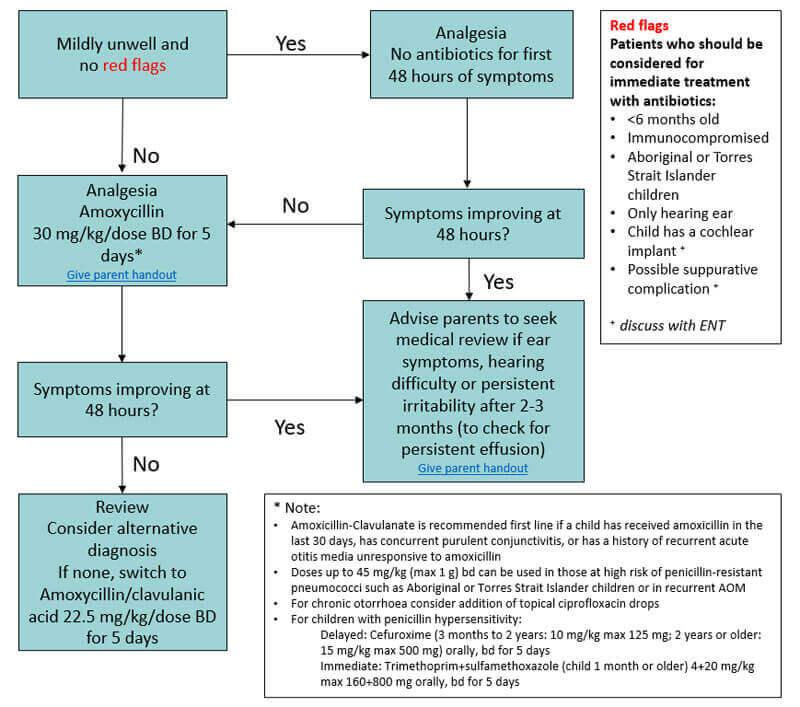
Medical management of ASOM
Pain management
Control of pain and pyrexia are important. Use age-appropriate analgesics and antipyretics.
First-line antibiotics
Watchful waiting can be used in selected children older than 6 months of age with nonsevere acute otitis while observing for clinical improvement in 24 to 48 hours. Not only appropriate antibiotics but also correct dose, frequency, and duration of therapy are all important.
No penicillin allergy
Amoxycillin is the drug of choice
- Dose - 45-60 mg/kg/day in 3 divided dose regime
- Dose - 75-90 mg/kg/day in 2 divided dose regime
Consider Amoxicillin-clavulanate if
- Concurrent purulent conjunctivitis
- Use of Amoxicillin within 30 days period
- Relapse of ASOM
- No clinical response to amoxicillin.
For those with a Penicillin allergy
- In type 1 - hypersensitivity, Cefdinir can be given.
- In Type 4 - Azithromycin can be given
Read below for a better understanding of penicillin allergy
Second-line antibiotics
- Second-generation cephalosporin - Cefuroxime,
- Third generation -Parenteral Ceftriaxone.
Duration of antibiotics
10 days duration for
- Children younger than 2 years of age
- Children with recurrent AOM or AOM with perforated Tympanic membrane
5 days duration for
Children 2 years of age or older with the uncomplicated disease.
Surgical Management
The surgical option of Myringotomies & Tympanocentesis is used to facilitate drainage and healing.
Indications for surgical management in ASOM
- Severe, refractory pain.
- Hyperpyrexia.
- Complications of AOM such as facial paralysis, mastoiditis, labyrinthitis, or central nervous system infection.
- Recurrent AOM despite adequate medical therapy.
Complications
1. Tympanosclerosis
2. Atelectasis of the TM - as a consequence of long-standing retraction or severe or chronic inflammation.
3. Retraction pocket is a localized area of atelectasis. A deep retraction pocket may lead to erosion of the ossicles and adhesive otitis and may serve as the nidus of a cholesteatoma.
4. Chronic perforation more commonly results as sequelae of CSOM, generally accompanied by conductive hearing loss.
5. Cholesteatoma formation.
6. Permanent conductive hearing loss.
7. Permanent sensorineural hearing loss with acute or chronic OM, secondary to spread of infection or products of inflammation through the round window membrane, or as a consequence of suppurative labyrinthitis.
8. Permanent hearing loss can cause delays in speech and language development.
References
- Antibiotic therapy for children with acute otitis media
- Acute otitis media - RCH Clinical Practice Guidelines
Image attribution - Source1: Dr. Emad Kayyam, Wikimedia commons
Author

Shailesh Gophane | DCH DNB Pediatrics
Shailesh completed his Pediatric residency from Port Trust Hospital Mumbai after completing DCH from J.J. Hospital, Mumbai
💡 Join the Discussion!
🩺 Help us refine this article — share corrections or additional information below. Let's elevate the accuracy of knowledge together! 💉💬