Febrile neutropenia in pediatric oncology
You are asked to attend a call at 5:00 am by the nurse looking afrer a ward patient. 'Patient spiked a fever of 38° C (100.4°F) one hour ago'. He/she received chemotherapy recently after a diagnosis of AML was made and is currently stable.
You can simply order paracetamol and move on
OR
You ask her to repeat another reading, and think .......
Could this be a febrile Neutropenia?
The repeat temperature is 38.2 C (100.8 F), but wait febrile Neutropenia is temperature of 38.3C. Don't be tricked, there are a few questions you need to ask before you move on
- Does 38° C define febrile neutropenia?
- What's his Absolute Neutrophil Count?
- Had he received transfusion in the last 6 hours?
- Is his primary disease is know to cause fevers?
Definition of febrile neutropenia in children
The definition has two components.
A. Fever in febrile neutropenia
- A single oral temp > 38.3° C (101 ° F) or
- A temperature of >38 ° C(100.4F) on two occasions separated by1 hour
So don't be tricked, If the temperature is 37-38°C, repeat the temperature in 1 hour to see if the above criteria of fever are met.
B. Neutropenia in febrile neutropenia
- ANC < 500/mm3
or - < 1000/mm3 and predicted to decline to< 500/mm
Let us continue with our case. You ordered a PS and these are the results
| WBC | 700 |
| PMN | 38% |
| Bands | 2% |
How to calculate absolute neutrophil count?
ANC = (Total WBC count) x (% of total neutrophils)
- Take total percent of neutrophils which includes % polys + % bands
- Convert percent to a decimal by dividing by 100.
- Example 40%= 40/100= 0.40
- Multiply this number by the total White Blood Cells (WBC)
- Here total neutrophils will be 38%+2% = 40% i.e 0.4
- ANC = 04 * 700 = 280
History taking in febrile Neutropenia
- What is a primary disease?
- Status of remission?
- History of splenectomy?. If present, think of Strep. Pneumoniae, Neisseria meningitides, Hemophilus influenza.
- Focused history of other organ systems
- Localizing symptoms suggesting a likely source for infection
- Immunization history
- History of comorbidities
- Enquire about in-dwelling catheters etc.
Chemotherapy history
- Drug history, steroids, any previous antibiotics.
- Allergies
Transfusion history
Oncology patients often receive blood transfusions that can cause fevers.
Physical Examination
Along with overall general examination focus on the following points in case of febrile neutropenia
- Oral cavity examination is important. Look for oral ulcers, examine the pharynx.
- Skin examination is important, Examine bone marrow aspirations sites, vascular catheter access sites, and tissue around the nails.
- Don't miss rashes from drug eruptions/herpes zoster reactivation / Petechial rashes all are common in these patients.
- Look for right lower quadrant tenderness for signs of Typhilitis
- Careful respiratory and abdominal examination since they are common sites of infection.
Note - In vitals, rectal temperature reading should not be taken as it compromises rectal mucosal integrity that can induce Gram-negative bacteremia with trauma. If you have an OSCE station - 'Perform focused examination in this case of febrile neutropenia. Mention - No rectal temperature checks!
Predicting neutropenia in oncology patients and why it is important?
This is important since you can predict when the fever can be likely to be febrile neutropenia. The duration and timeline of chemo, therefore, become an important part of history taking.
- Most chemotherapy agents/protocols cause neutropenia nadir at 10-14 days.
- But can be see anytime from a few days after chemotherapy to up to 4-6 weeks later depending on the agents used
Severity of neutropenia
- Normal ANC 1500 to 8000 cells/mm3
- Neutropenia: ANC < 1500 cells / mm3
- Mild Neutropenia: 1000-1500 cells/ mm3
- Moderate Neutropenia: 500-999 cells/mm3
- Severe Neutropenia: < 500 cells / mm3
- Profound Neutropenia: <100 cells/ mm3
Severity of neutropenia and risk of Infections
- 20-30% of patients with ANC <100 cells/mm3 with febrile neutropenia episodes have bacteremias. (NEJM, 1971;284:1061)
- 50 % of Pseudomonas Aeruginosa Bacteremia results in death within 72 hours when ANC is < 1000.
Duration of Neutropenia and risk of infection
Neutropenia lasting for < 7 days low risk
- 30% develop fever or infection when neutropenia last <7 days
- Response rates to initial antimicrobial therapy is higher
Neutropenia lasting for >7 days high risk
- 100% develop fever or infection when it remains low for > 7 days.
- Response rate to antimicrobials is lower
Common Organism causing infection in Febrile neutropenia
Gram-positive infections are dominant, however, gram-negative infections have shown significant resurgence.
Gram positive cocci and bacilli
- Staph. aureus
- Staphylococcus epidermidis
- Entercoccus
- Cornybacterium species
Gram-negative organism
- Escherichia coli
- Klebsiella species
- Pseudomonas aerugenosa
Fungi
- Candida- Nonalbicans (emerging)
- Aspergillus are more common in HSCT
Viruses
Respiratory infections with viruses are commonly seen that include
- Influenza, RSV
- Parainfluenza
- Rhinovirus
- Adenovirus
- Coronaviruses.

|
| Febrile neutropenia -Image source1 |
Investigations
Hematology
- Complete Blood Count with Differential
- Peripheral smear
Biochemistry
- Electrolytes
- Renal and liver function
- Other organ functions
Microbiology
- Blood cultures, peripheral and all central line lumens
- CSF for culture
- Oral ulcers or sores - send swabs ( Viral Cx and fungal Cx )
- Exit site swabs
- Wound swabs
- Urine Cultures (SSx/Foley Catheter)
- Stool Cultures and CDiff Toxin/PCR
Examination of CSF specimens is not recommended as a routine procedure but should be considered if a CNS infection is suspected and thrombocytopenia is absent or manageable.
Aspiration or biopsy of skin lesions suspected of being infected should be performed for cytologic testing, Gram staining, and culture.
Radiology/Imaging
- CXR if Symptomatic or if out pt Rx considered
- High-resolution CT Chest Indicated ONLY if persistent fevers with pulmonary symptoms even after initiation of empiric Abx
- CT abdomen for Necrotizing Enterocolitis or Typhilitis
- CT brain to rule our ICH
- MRI of the spine or brain for evaluation of metastatic disease than febrile neutropenia itself.
Risk stratification in children with febrile neutropenia
Pediatric patients can be classified as high-risk or low-risk categories.
1. Neutropenia
- Increased risk with the severity of neutropenia (< 100/mm)
- Duration of neutropenia (> 7 days)
2. Bacteremia
- Gram-negative > gram-positive
3. Underlying malignancy
- Acute Leukemia - Read more
- Relapsed disease Solid-organ malignancies: Local effects eg obstruction, Invasion
- Presence of co-morbidities
- Age >60
- Hemodynamic instability
- Oral or gastrointestinal mucositis that interferes with swallowing or cause severe diarrhea
- GI symptoms eg. Nausea, vomit, abdominal pain
- Neurological or mental status change of new-onset
- Intravascular catheter infection, catheter tunnel infection New pulmonary infiltrates or Hypoxemia, underlying chronic lung disease
- Evidence of hepatic insufficiency or renal insufficiency
Risk stratification scores
There are several models/scores for risk stratification.
The MASCC Risk Index score is a validated scoring system that identifies low risk patients that can potentially be treated as an outpatient with early antibiotics.
| No or Mild symptoms | 5 |
| Moderate symptoms | 3 |
| No Hypotension | 5 |
| No COPD | 4 |
| Solid tumour/Haem malignancy (no fungal infection) | 4 |
| Outpatient | 3 |
| No dehydration | 3 |
| Age <60 yrs low risk is score>20 | 2 |
Management of febrile neutropenia in children
The treatment is based upon risk stratification
Mild cases
For patients who are at low risk for developing infection-related complications during the course of neutropenia, oral antibiotics can be given at home.
Use if
- The patient is able to tolerate and absorb orally
- The ability of caregiver to monitor at home
- Contact and transportation support is readily available
- A combined decision of patient/caregiver and pediatrician has been made
Oral antibiotics for treatment of febrile neutropenia
- Oral ciprofloxacin plus amoxicillin/clavulanate
- Oral ciprofloxacin plus clindamycin for penicillin allergy
Empirical IV antibiotic therapy
Empirical therapy is very important and should be initiated immediately (within 1 hour) after blood cultures have been taken. However, for some reason, this is not possible, the antibiotics should not be delayed. (surviving sepsis guideline).
Later the antimicrobial therapy should be managed according to culture and sensitivity of organism/IV empirical therapy
- IV Monotherapy
- IV Dual therapy
- IV Combination therapy
1. Monotherapy
One of the following is used as empirical therapy
- Extended-spectrum Anti pseudomonal Cephalosporins
- Cefepime
- Ceftazidime
- Carbapenem
- Imipenem -Cilastatin
- Meropenem
- Anti pseudomonal penicillins
- Piperacillin- Tazobactam
- Ticarcillin- Clavulanic acid
2. Dual therapy
- For Gm -ve organisms: B lactam / carbapenem + Aminoglycoside / fluoroquinolones
- For respiratory infection: B lactam / carbapenem + Aminoglycoside / fluoroquinolones for 10-14 days
- Oral ulcerations or esophagitis may point toward HSV or Candida esophagitis infections in high-risk patients, therefore empirical antiviral (acyclovir) and/or antifungal (fluconazole) should be used.
Routine use of antifungals is not recommended in low-risk patients
3. Combination Therapy
This simply is combining Vancomycin with mono or dual therapy
Indications for Vancomycin in febrile neutropenia in children.
- Clinically suspected serious catheter-related infections/skin soft tissue infection
- known colonization with penicillin- and
cephalosporin-resistant pneumococci strep. Viridance or
MRSA, ( FOR VRE add linezolide) - Positive results of blood culture for gram-positive
- Hemodynamic instability ie. hypotension or other evidence of cardiovascular impairment
- H/O ciprofloxacin or trimethoprim-sulfamethoxazole
- Pneumonia documented radiographically
Treatment of vancomycin-resistant enterococcus (VRE) in febrile neutropenia
- Linezolid (can cause bone marrow suppression)
- Daptomycin
- Quinopristin- Dalfopristin (can cause severe arthralgia)
Remember VRE is an independent risk factor for death in febrile neutropenia
Penicillin allergy in febrile neutropenia
If non-allergic to cephalosporin
- Cefepime
If allergic to cephalosporin
- Use Aztreonam +/- Aminoglycoside or a Fluroquinolone
Add +/- Vancomycin if indicated
Pearls
- Monitor drug(antibiotics)
- Ensure that empirical antibiotics are tolerated and the patient remains stable during the course of outpatient-based therapy
- Add aminoglycoside and timely switch to carbapenem for pneumonia for gm-ve bacteremia
- Use Metronidazole for abdominal symptoms or suspected C. Difficle infection
Monitoring progress
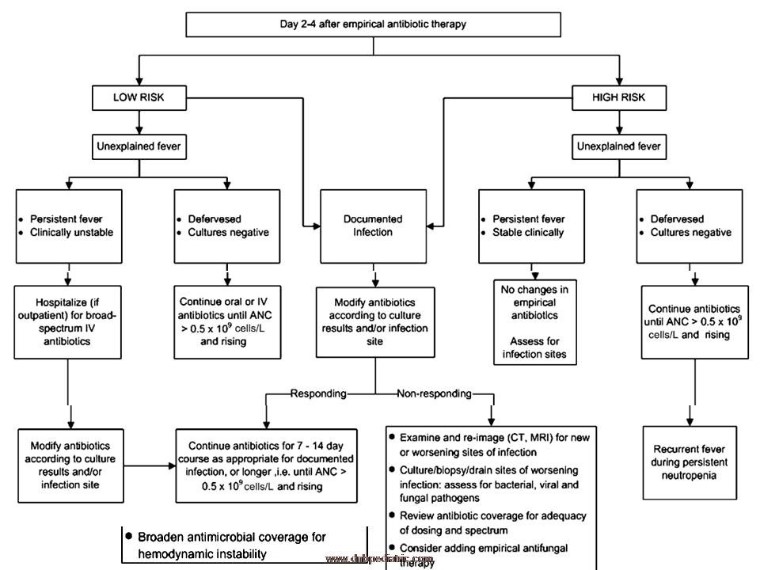 |
| Febrile neutropenia follow up |
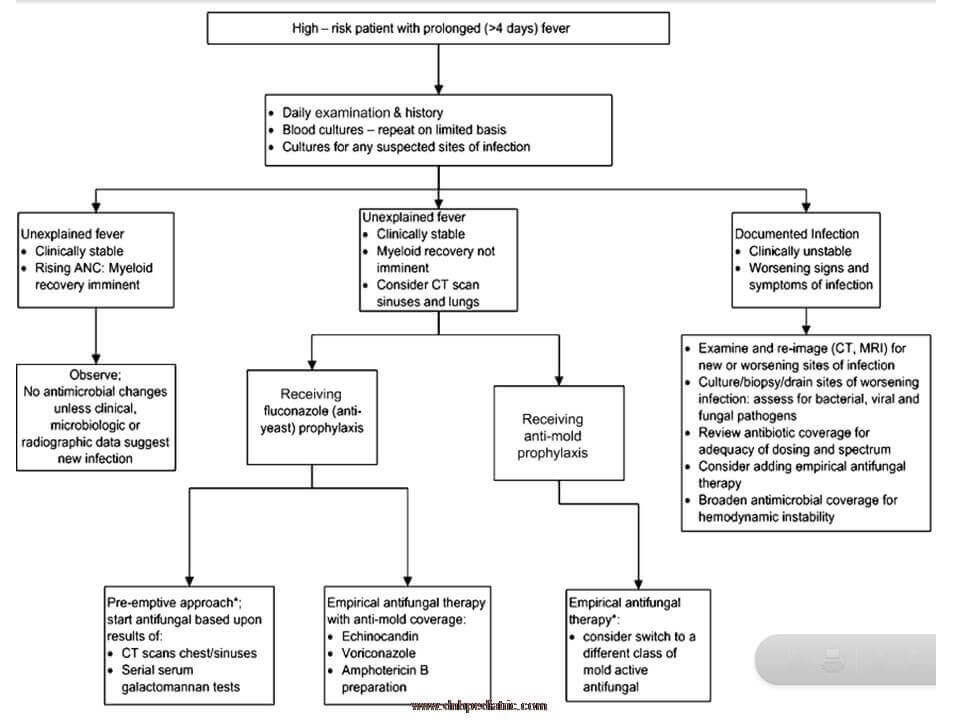
|
| Febrile neutropenia follow up - high risk |
Prophylaxis in febrile neutropenia
Antibiotic and antifungal prophylaxis
- Not indicated for the low-risk patients.
- Fluoroquinolone prophylaxis should be considered for high-risk patients with expected durations of prolonged and profound neutropenia (ANC <100 cells/mm3 for 7 days). Levofloxacin or ciprofloxacin can be used for this
- Allogeneic HSCT/ intensive remission induction/ salvage induction agent use: Prophylaxis against Candida infection is recommended. Fluconazole, itraconazole, voriconazole, posaconazole, micafungin, and caspofungin are all acceptable.
- Invasive Aspergillus infections with posaconazole should be considered for selected patients > 13 years of age who are undergoing intensive chemotherapy for hematological malignancy in whom the risk of invasive aspergillosis without prophylaxis is substantial
a mold-active agent is recommended in patients with prior invasive aspergillosis, anticipated prolonged neutropenic periods of at least 2 weeks, or a prolonged period of neutropenia immediately prior to HSCT.
Anti viral prophylaxis
- HSV seropositive patient undergoing transplant
- Yearly inactivated influenza vaccination to all > 7 days after or > 2 wk prior to chemotherapy treat influenza with neuraminidase inhibitor in the outbreak.
G-CSF/GM CSF prophylaxis in febrile neutropenia
Prophylactic use of colony-stimulating factors should be considered for patients in whom the
- Anticipated risk of fever and neutropenia is 20%or more.
- CSFs are not generally recommended for the treatment of established fever and neutropenia.
Duration of antibiotic therapy
1 week of antibiotics if
- Afebrile by day 3
- Neutrophils >500/mm3 (2 consecutive days) Cultures negative
- Low-risk patient, uncomplicated course
>1 week of antibiotics if
Temps slow to settle (>3 days)
Continue for 4-5 days after neutrophil recovery (>500/mm3 )
2 weeks of antibiotics if
- Bacteraemia, deep tissue infection
- After 2 weeks if remains neutropenic ( < 500/mm3), BUT afebrile, no disease focus, mucous membranes, skin intact, no catheter site infection, no invasive procedures or ablative therapy planned.
When to stop antibiotics in febrile neutropenia?
1. Documented Infection
- 10-14 days/ till ANC>500
- Clinical and microbiologically settled
2. Unexplained Fever in Low-Risk Patients
- An ANC >500 cells/mm3 if cultures are negative at 48 hours and patients remain afebrile for at least 24 hour
- The daily increase in the absolute phagocyte count (bands and mature neutrophils combined), the absolute monocyte count, or the reticulocyte fraction
- In low-risk patients who have effervesced after 3 days of empirical antibiotic therapy, evidence of imminent marrow recovery may direct cessation of broad-spectrum antibiotics prior to the ANC reaching 500 cells/mm3
3. Unexplained high risk
- Early discontinuation of antibiotic therapy, while fever and neutropenia both persist, is strongly discouraged for high-risk patients.
- Some experts advocate that patients with unexplained fever who remain afebrile for 4-5 days may have empirical antibiotics switched back to fluoroquinolone prophylaxis for the remaining duration of neutropenia
The persistent temperature in febrile neutropenia
Reasons
- Non-bacterial infection (eg fungal, viral)
- Superinfection
- Cell wall deficient bacteria (eg Mycoplasma, Chlamydia)
- Infection at an avascular site (abscess or catheter)
- Primary disease-related fever
- Bacterial resistance to first-line therapy (MRSA, VRE)
- Slow response to drugs in use
- Inadequate antibiotic dose
- Drug fever
Antifungals in febrile neutropenia
Pearls
- Easy to Initiate but difficult to stop
- Aggressively search for fungal Infection.
- Keep low threshold for CT Chest and Abdomen, CT Sinuses in high-risk group.
Antifungal agents
Amphotericin B
- Amphotericin B is an IV drug of choice for high-risk patients.
- Alternative options are FLUCONAZOLE, ITRACONAZOLE, ECHINOCANDINS, Voriconazole
Fluconazole
- Fluconazole is acceptable if there is no clinical/microbiological evidence of molds and resistant Candida infection like C. Krusei and C.glabrata.
- Also can be used orally in low-risk patients
Do not use Fluconazole
- If there is evidence of sinusitis or radiographic evidence of pulmonary disease.
- If the patient has received Fluconazole prophylaxis before.
Itraconazole
Recent studies show equal efficacy of Itraconazole when compared to amphotericin B.
Prevention of infection in febrile neutropenia
The most important thing in febrile neutropenia is the prevention of infection by following
- Hand hygiene
- Standard barrier precautions
- Plants and dried or fresh flowers should not be allowed in the rooms of hospitalized neutropenic patients.
- Hospital staff sickness and exposure reporting should be encouraged.
- Isolation and air exchange room when necessary.
- 12 air exchanges/hour and high-efficiency particulate air (HEPA) filtration.
References
- Febrile Neutropenia - Peds cases
- Febrile Neutropenia - Learn pediatrics
- 2021 update (pdf) on febrile neutropenia
- Guideline for the Management of Fever and Neutropenia in Children with Cancer and/or Undergoing Hematopoietic Stem-Cell Transplantation
- Etiology and Clinical Course of Febrile Neutropenia in Children with Cancer. J Pediatr Hematol Oncol. 2009 Sep; 31(9): 623–629. doi: 10.1097/MPH.0b013e3181b1edc6
- Febrile neutropenia in paediatric oncology. Paediatr Child Health (Oxford). 2020 Mar; 30(3): 93–97.
- Gaur AH, Giannini MA, Flynn PM, et al. Optimizing blood culture practices in pediatric immunocompromised patients: evaluation of media types and blood culture volume. Pediatr Infect Dis J. 2003 Jun;22(6):545–552.
- Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of America. Clin Infect Dis. 2011 Feb 15;52(4):e56-93. doi: 10.1093/cid/cir073.
Author

Hemang Mendpara | DNB(pediatrics), Fellowship(Pediatric Intensive Care)
Hemang completed Pediatric residency from CHRC, Indore and received further training in PICU.
Author

Ajay Agade | DNB(Pediatrics), FNB(Pediatric Intensive Care), Fellowship in Pediatric pulmonology and LTV
Ajay is a Paediatric Intensivist, currently working in Pediatric Pulmonology & LTV at Great Ormond Street Hospital NHS, London
💡 Join the Discussion!
🩺 Help us refine this article — share corrections or additional information below. Let's elevate the accuracy of knowledge together! 💉💬