Pathophysiology of functional constipation in children
This guide will cover
- Definition of functional constipation
- Rome IV criteria for functional constipation
- Theories proposed for functional constipation
- Pathophysiology of functional constipation
- Withholding behavior in details
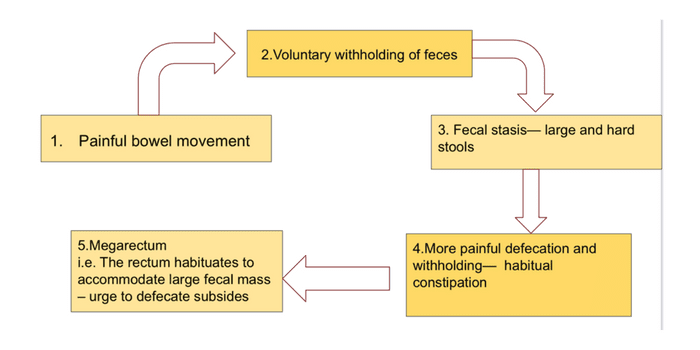
- Flow diagrams useful for exam
Frequently asked questions
- Pathophysiology of Functional constipation - Dec 2021
- Treatment of Functional constipation - June 2021
What is functional constipation?
Constipation is broadly defined as the painful or incomplete evacuation of hard stools often characterized by infrequent stools.
Constipation is functional if there is no underlying organic cause.
Rome IV diagnostic criteria for functional constipation in children
Infants and toddlers up to 4 years old
| At least 2 of the following present for at least 1 month: |
| 2 or fewer defecations per week |
| History of excessive stool retention |
| History of painful or hard bowel movements |
| History of large-diameter stools |
| Presence of a large fecal mass in the rectum |
| In toilet-trained children, the following additional criteria may be used: |
| At least 1 episode/week of incontinence after the acquisition of toileting skills |
| History of large-diameter stools that may obstruct the toilet |
Children and adolescents (developmental age ≥4 years)
| At least 2 of the following present at least once per week for at least 1 month + Symptoms are insufficient to fulfill the diagnostic criteria of irritable bowel syndrome |
| 2 or fewer defecations in the toilet per week |
| At least 1 episode of fecal incontinence per week |
| History of retentive posturing or excessive volitional stool retention |
| History of painful or hard bowel movements |
| Presence of a large fecal mass in the rectum |
| History of large-diameter stools that may obstruct the toilet |
| The symptoms cannot be fully explained by another medical condition |
Pathophysiology of functional constipation
The pathophysiology of functional capacity in children remains unclear but is multifactorial. 3 Most commonly discussed theories are
- Withholding behaviour
- Slow transit
- Genetic factors
The most common mechanism for developing FC, especially in younger age group, is withholding behavior.
Withholding behaviour
The physiology of functional constipation can be explained based on three events.
- Initial events
- Cycles of fecal stasis
- Stool-withholding maneuver
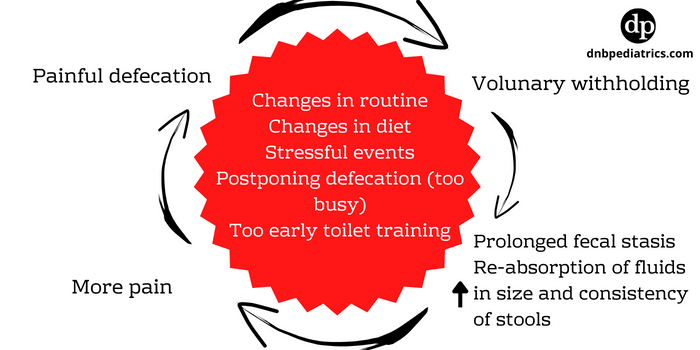
Events/causes that lead to initial painful defecation and later develop as functional constipation
- Change in routines like the timing of defecation or diet, starting of school.
- Stressful events like physical or sexual abuse
- Inter-current illnesses,
- Non-availability of toilets such as long and frequent travels.
- Child’s postponing defecation because he or she is too busy (morning school, play)
- Forceful toilet training (too early, too harsh).
All these events give rise to large, hard stool and the passage of such stools lead to stretching of the pain-sensitive anal canal. As a result of this child decides to avoid defecation.
Cycles of fecal stasis
Withholding of feces leads to prolonged fecal stasis in the rectum, with the resultant absorption of fluids and harder stools.
Successive retention of stools in the rectum makes them larger.
As the cycle is repeated, successively greater amounts of larger and harder stools are built up in the rectum and passed with even greater pain accompanied by severe “stool withholding maneuvers”.
Thus a vicious cycle sets in
Stool-withholding maneuver
These children develop a “stool-withholding maneuver” or retentive posture which parents mistakenly think it as an attempt to defecate.
They refuse to sit on the toilet, rather rise on their toes, hold their legs and buttocks stiffly, and often rock back and forth, holding on to furniture, screaming, and turning red until a bowel movement finally takes place.
Eventually, liquid stool from the proximal colon may percolate around these hard stools and pass per rectum involuntarily ( fecal incontinence).
With more and more stasis, the rectum becomes dilated and redundant, and the sensitivity of the defecation reflex and the effectiveness of peristaltic contractions of rectal muscles decrease.
Other proposed theories for functional constipation
Slow Transit
The interstitial cells of Cajal play an important role in gut motility. These cells act like pacemakers that generate gut peristalsis.
In some children, Functional constipation can result from low number of interstitial cells of Cajal without any other signficant pathological.organic findings.
Genetic factors for functional constipation
Many children with functional constipation have a positive family history. In this subgroup genetic factors may play a role. Neurodevelopmental disorders such as autism spectrum disorders (ASDs) can be associated with functional constipation resulting from lack of adequate behavioral response to a defecation sensation.
More in Gastro-enterology
Author

Gaythri G | DNB Pediatrics
Gayathri is DNB in Pediatrics. She has completed her residency from Meenakshi mission hospital and research centre, Madurai
1 comment
🩺 Help us refine this article — share corrections or additional information below. Let's elevate the accuracy of knowledge together! 💉💬