Pediatric Stroke | Features, Diagnosis and management
This guide covers stroke in children and outlines its types, causes, clinical features, approach, diagnosis, differentials, and management. Stroke is an important cause of acquired brain injury in newborns and children. It is also one of the most frequently asked questions in theory and as a clinical case.
Commonly asked questions. This guide covers the following questions.
- Pediatric stroke management. (2021/02)5
- Diagnostic evaluation of stroke(2020/01)5
- Causes and investigations in a child with stroke (1/2016)5
- Enumerate the causes of stroke in children. Discuss the diagnostic approach for managing a child with stroke. (2011/2)3+7
- What are the causes of hypercoagulable states in children? How will you manage a case of acute hemiplegia? (2009/2)4+6
- Describe the causes of arterial thromboembolism in children. Outline the management of a child with acute hemiplegia. (2008/1)10
- Briefly discuss the arterial supply of the Brain. Outline the causes of acute hemiplegia in a 2 year old child (2007/2)10
- Discuss the etiopathogenesis, clinical symptomatology and differential diagnosis of childhood stroke (2006/2)10
- Discuss the etiopathogenesis of acute onset hemiplegia in a 3 year old child. How will you manage this child? (2004/2)4+6
- Stroke in childhood (2000/1)15
Table of Contents
Types
- Ischemic
- Arterial ischemic stroke (AIS)
- Cerebral sinovenous thrombosis (CSVT)
- Hemorrhagic
- Hemorrhagic stroke and
- Cerebrovascular disease.
Causes for arterial ischemic stroke
- Arterio-pathic
- Focal cerebral arteriopathy
- Transient cerebral arteriopathy
- Moyamoya
- Arterial infection
- Migraine
- Cardiac
- Complex cyanotic heart disease
- Cardiac procedures
- Arrhythmias
- Endocarditis
- Cardiomyopathy
- Genetic
- Hereditary dyslipoproteinemia
- Heritable disorders of connective tissue
- Organic acidemias
- Mitochondrial encepahalomyoapthies
- Haematological
- Sickle cell anemia
- Iron deficiency anemia
- Inherited prothrombotic states such as
- factor V Leiden,
- prothrombin gene mutation
- Acquired prothrombotic states such as
- Protein C/S deficiency,
- antithrombin III deficiency,
- antiphospholipid antibodies,
- oral contraceptives,
- pregnancy
Causes of hemorrhagic stroke
- Vascular disorders
- Arteriovenous malformations
- Cavernous malformations (cavernomas)
- Venous angiomas
- Hereditary hemorrhagic telangiectasia
- Intracranial aneurysm
- Choroid plexus angiomas
- Drugs/ toxins
- Blood disorder
- Idiopathic thrombocytopenic purpura
- Hemolytic uremic syndrome
- Hepatic disease/failurecoagulopathy
- Vitamin K deficiency(hemorrhagic disease of the newborn)
- Disseminated intravascular coagulation
- Trauma
- Middle meningeal artery injury
- Bridging vein injury (subdural hematoma)
- Subarachnoid hemorrhage
- Hemorrhagic contusions (coup and contrecoup)
- Nonaccidental trauma
- Iatrogenic(neurosurgical procedures,angiography)
Arterial Blood supply of brain

|
| Fig 1. Circle of Willis |
Two main sources of supply are
- Internal carotid arteries
- Vertebral arteries.
The internal carotid arteries branch to form two major cerebral arteries, the anterior and middle cerebral arteries.
The right and left vertebral arteries join together and form the basilar artery.
The basilar artery then joins the internal carotids and forms a vascular ring at the base of the brain called the circle of Willis
Anterior cerebral artery supplies
Portions of the frontal lobe and most of the superior-medial parietal lobes.
Middle cerebral artery supplies
Majority of the lateral surface of the cerebral hemispheres, deep structures like Broca's area and Wernicke area, and the temporal lobes of the brain.
It is the largest cerebral artery and is also most commonly affected.
Posterior cerebral artery supplies
The occipital lobe, the inferior part of the temporal lobe, and deep structures such as the thalamus and the posterior limb of the internal capsule.
Clinical Features
The acute onset of a focal neurologic deficit in a child is stroke until proven otherwise.
Arterial ischemic stroke (AIS)
The most common focal presentation is hemiparesis but acute visual, speech, sensory, or balance deficits also occur.
Children with these presentations require urgent neuroimaging and consultation with a child neurologist as emergency interventions may be indicated.
Hemorrhagic stroke (HS)
Clinical presentations vary according to location, cause, and rate of bleeding. Acute hemorrhages may feature instantaneous or thunderclap headaches, loss of consciousness, nuchal rigidity, focal neurologic deficits, and seizures.
Hemorrhagic stroke can be rapidly fatal.
In bleeds associated with vascular malformations - pulsatile tinnitus, cranial bruit, and high-output heart failure may be present.
Investigation
Neuroimaging
Role of Neuroimaging in stroke
- To differentiate ischemia from bleed.
- Define the extent of the lesion
- Identify potential cause
- Help select the treatment line
CT
CT is particularly useful in acute emergency situations and imaging in a patient with unstable hemodynamics.
CT perfusion and CT angio is used. CT without contrast is not of much use.
CT is highly sensitive to acute HS and can rule out hemorrhagic stroke with accuracy. CT can demonstrate larger mature acute hemorrhagic stroke (AIS).
MRI
MRI identifies early and small infarcts and is therefore required to exclude ischemic stroke. MRI is also highly sensitive to even small amounts of acute hemorrhage.
Diffusion-weighted MRI (DWI) can demonstrate AIS within minutes of onset.
MR angiography can confirm vascular pathology such as occlusion and can help to identify the cause.
Angiography
Angiography by CT, MR, or conventional means is often required to exclude underlying vascular abnormalities.
Neuroimaging findings
CT: Hyperdense region surrounded by edema, Intraventricular hemorrhages
CT Venography: Filling defects
MRI: Focal increased diffusion, multifocal and restricted diffusion. Demyelination. Follow-up MRI may show atrophy/ gliosis.
MR Angiogram: occlusion, stenosis, decreased flow, puffed smoke appearance (moya moya disease), aneurysms, and vascular malformations can be seen.
MR Spectroscopy: Increased lactate peak in MELAS-related stroke.
Other
Cardiac ECHO
Can help rule out cardiac embolus as a cause of ischaemic stroke.
Hb
Monitoring Hemoglobin, in hemorrhagic stroke will guide on progress as well as supportive therapy
Coagulation profile testing, Protein C and S levels
Deficient Protein C and S levels can lead to abnormal clotting and ischaemic stroke.
Approach to pediatric stroke
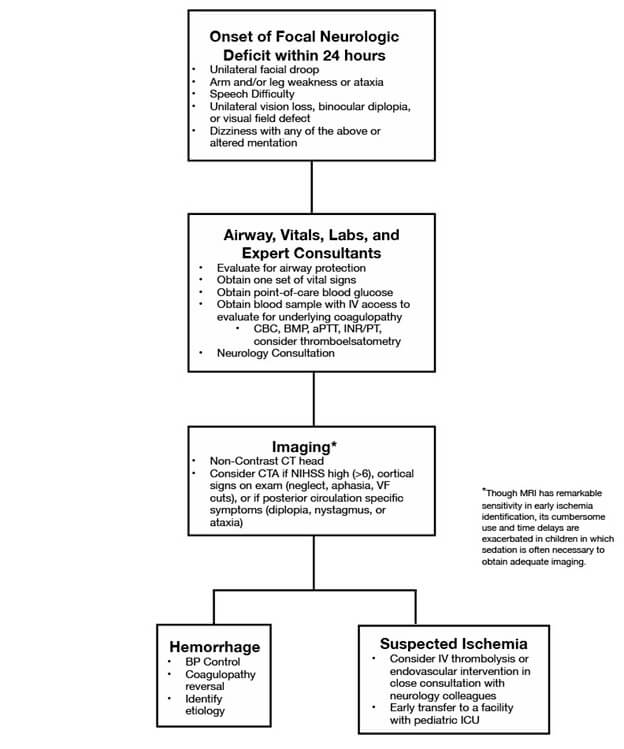
|
| Approach to a child with a stroke |
Treatment
- Antithrombotic strategies - Heparin can be used for acute situations. Warfarin, aspirin and clopidogrel are used for the maintenance and prevention of clotting.
- Neuroprotective strategies - Raised ICP should be promptly controlled by antiedema measures if present. Control of seizures, blood glucose, and temperature for prevention of raised ICP and secondary brain injury
- Disease-specific treatment - Transfusion in sickle cell and iron def anemia. Reversal of anticoagulant therapy may be required (e.g., vitamin K, fresh frozen plasma). The role of factor VII is unstudied. Immunosuppression in vasculitis.
- Surgery - Emergent neurosurgical intervention for large or rapidly expanding lesions is important. Moyamoya disease will require surgical intervention.
- Rehabilitation - A multidisciplinary approach involving a Pediatrician, neurologist, physiotherapist, and psychological support should be offered.
Differential diagnosis of stroke-like disorders in children
| Disorder | Clinical distinction from stroke | Imaging distinction from stroke |
| Migraine | Evolving or “marching” symptoms, short duration, complete resolution, headache, personal or family history of migraine | Typically normal Migrainous infarction is rare |
| Seizure | Positive symptoms, Todd's paralysis is post-seizure and limited | Normal or may identify the source of seizures (e.g., malformation, old injury) |
| Infection | Fever, encephalopathy, gradual onset, meningismus | Normal or signs of encephalitis/cerebritis, which are typically diffuse and bilateral |
| Demyelination | Gradual onset, multifocal symptoms, encephalopathy Accompanying optic neuritis | Multifocal lesions, typical appearance (e.g., patchy in ADEM, ovoid in MS), |
| Hypoglycemia | Risk factors (e.g., insulin therapy), related to meals, additional systemic symptoms | Bilateral, symmetric Posterior dominant pattern |
| Watershed infarction due to global HIE | Risk factors (e.g., hypotension, sepsis, heart disease), bilateral deficits | Bilateral, symmetric restricted diffusion in border zones between major arteries (watersheds) |
| Hypertensive encephalopathy (PRES) | Documented hypertension, bilateral visual symptoms, encephalopathy | Posterior dominant, bilateral, patchy lesions involving gray and white matter |
| Inborn errors of metabolism | Pre-existing delays/regression, multisystem disease, abnormal biochemical profiles | MR spectroscopy changes (e.g., high lactate in MELAS) |
| Vestibulopathy | Symptoms limited to vertigo, imbalance (i.e., no weakness) Gradual onset | Normal |
| Acute cerebellar ataxia | Sudden onset bilaterally symmetric ataxia postviral | Normal |
| Channelopathy | Syndromic cluster of symptoms not localizing to a single lesion Gradual onset, progressive evolution | Normal |
| Alternating hemiplegia | History contralateral events Choreoathetosis/dystonia | Normal |
| You can use the following pneumonic to remember the differentials. MIS W HAD A/C HIV (Mis world had acute on chronic HIV) - Migraine, infections, seizure, watershed infarcts due to HIE, hypoglycemia, ataxia, demyelination, alternating hemiplegia, channelopathies, HTN, IEM, vestibulopathy. |
Further reading
- Stroke in childhood. RCPCH Clinical guideline for diagnosis, management and rehabilitation. [ext link]
- Hollist M, Au K, Morgan L, Shetty PA, Rane R, Hollist A, Amaniampong A, Kirmani BF. Pediatric Stroke: Overview and Recent Updates. Aging Dis. 2021 Jul 1;12(4):1043-1055. doi: 10.14336/AD.2021.0219. PMID: 34221548 [ext link]
Attribution
- Fig 1. - Rhcastilhos, Public domain, via Wikimedia Commons.
- Fig 2. - Hollist M, Au K, Morgan L, Shetty PA, Rane R, Hollist A, Amaniampong A, Kirmani BF. Pediatric Stroke: Overview and Recent Updates. Aging Dis. 2021 Jul 1;12(4):1043-1055. doi: 10.14336/AD.2021.0219. PMID: 34221548.
{kind=link}
Author

Vasu Burli | DNB (Pediatrics), Fellowship in Pediatric Critical Care
Vasu completed his Pediatrics residency at Kanchi KamaKoti Childs Trust Hospital, Chennai and received further training in Pediatric Intensive care in India and UK
💡 Join the Discussion!
🩺 Help us refine this article — share corrections or additional information below. Let's elevate the accuracy of knowledge together! 💉💬