Pediatric Burns | Classification and management
Table of Content
- Classification of burns
- Clinical manifestation of electrical burns
- Emergency management
- Fluid resuscitation
- Goals of fluid resus
Related Question
- Provide a classification of burns injury. Describe the clinical manifestation of electrical burns. Outline the emergency management of a child with 20% burns.
Classification of Burn Injuries based on the depth
A. 1st-degree burns
Involves only the epidermis and are characterized by swelling, erythema, and pain (similar to mild sunburn). Tissue damage is usually minimal, and there is no blistering. Pain resolves in 48-72 hr; in a small percentage of patients, the damaged epithelium peels off, leaving no residual scars.
B. 2nd-degree burn
Involves injury to the entire epidermis and a variable portion of the dermal layer (vesicle and blister formation are characteristic).
- A superficial 2nd-degree burn is extremely painful because a large number of remaining viable nerve endings are exposed. Superficial 2nd-degree burns heal in 7-14 days as the epithelium regenerates in the absence of infection.
- Midlevel to deep 2nd-degree burns also heal spontaneously if wounds are kept clean and infection-free. Pain is less when compared to more superficial burns because fewer nerve endings remain viable. Fluid losses and metabolic effects of deep dermal (2nd-degree) burns are essentially the same as those of 3rd-degree burns.
C. Full-thickness, or 3rd-degree burns
These involve the destruction of the entire epidermis and dermis, leaving no residual epidermal cells to repopulate the damaged area. The wound cannot epithelialize and can heal only by wound contraction or skin grafting. The absence of pain sensation and capillary filling demonstrates the loss of nerve and capillary elements.
Clinical manifestation of electrical burns
1. Cardiac Dysrhythmias:
Arrhythmias are most common including, life-threatening cardiac arrest, asystole, ventricular fibrillation, sinus tachycardia, sinus bradycardia, premature atrial contractions (PACs), premature ventricular contractions (PVCs), conduction defects, atrial fibrillation, etc. ST-T wave changes are also seen.
2. Pulmonary
Respiratory arrest, acute respiratory distress syndrome
3. Renal:
ARF, Myoglobinuria
4. Neurologic
Immediate concerns
- Loss of consciousness
- Motor paralysis,
- Visual disturbances,
- Amnesia,
- Agitation;
- Intracranial hematoma.
- Paraplegia, brachial plexus injury,
- Syndrome of inappropriate antidiuretic hormone secretion (SIADH)
- Autonomic disturbances
- Cerebral edema
Delayed Complications
- Paraplegia
- Seizures
- Headache
- Peripheral neuropathy
- Cutaneous/oral/commissure burns
- Tongue and dental injuries
- Skin burns resulting from ignition of clothes
- Entrance and exit burns
4. Abdominal Viscus
Abdominal injury is rare without visible abdominal burns.
- Perforation and solid organ damage
- Ileus
5. Musculoskeletal
Compartment syndrome can result from subcutaneous necrosis, limb edema and deep burns.
6. Ocular and Visual Injuries
- Optic neuritis
- Cataracts
- Extra-ocular muscle paresis
Emergency management of a child with 20% burns
Initial resuscitation covers
- Establishing airway
- Ensuring breathing support if needed
- and Circulatory support
Make sure the patient and the carer are in a safe environment before commencing the emergency management.
Emergency management includes
Rapid review+ABC+Fluid resuscitation+Wound care+Triage
- Rapid review of all systems, rule out associated injuries
- Adequate fluid resuscitation to avoid organ injuries secondary to hypovolemia
- Cleaning the burnt surface if possible ( like tar, chemical) and prevention of infection by aseptic handling and sterile covers
- Pain management
- Provision of calorie requirements/nutrition wherever feeding is not contraindicated. this is really important since beginning in burns.
- Maintaining Normothermia
- Early Triage and hospitalization to appropriate facility like, burns unit, PICU, HDU or referral to another center whichever applicable.
Emergency Fluid Resuscitation in the child with 20%BSA
The Parkland formula estimates the fluid requirements for children with burns in the first 24 hours.
4 ml/kg of body weight in adults, this number is sometimes mentioned as 3 ml/kg in children per percentage burn of total body surface area (%TBSA) of crystalloid solution over the first 24 hours of care.
Calculate burns surface area using the rule of nine or charting on Lund-Browder diagram for estimating the extent of burns. Watch the following video on why the rule of nine can be misleading in children and details about parkland formula including issues with overestimating fluid resuscitation.

So based on this 3 to 4 mL/kg/20% BSA of lactated Ringer solution in 24 hours is required. Half of the fluid is given over the first 8 hr, calculated from the time of burns. The remaining fluid is provided over the next 16 hr.
Note, that the first 8 hours of fluid therapy start from the time of burn injury, thus, the first half of the total fluid may need to be administered at a faster rate if the patient has a delayed time before evaluation
For example, if a patient presents to a hospital 4 hours after a burn injury, then they should receive the first half of their fluids within 4 hours instead of 8 hours.
Parkland formula is just a beginning guide to fluid therapy in burns. The fluid requirement should be reassessed based on the initial response and criteria like urine output, heart rate blood pressure and can be modified. In children, maintenance fluid should alos be given using holiday-segars formula.
Consider fluid bolus of 10ml/kg in case of reduced perfusion based on vitals and clinical signs. If any boluses are given, do not forget to reduce the amount from the resus fluid.
Watch for hypoglycemia in children and add dextrose accordingly.
Goals of fluid reuscitation in Burns
- Pulse and blood pressure should return to age-appropriate values, and an adequate urine output (>1 mL/kg/hr in children; 0.5-10 mL/kg/hr in adolescents should be accomplished.
- Vital signs, acid-base balance, and mental status reflect the adequacy of resuscitation.
- All high-tension and electrical injuries require venous access to ensure forced alkaline diuresis in case of muscle injury to avoid myoglobinuric renal damage.
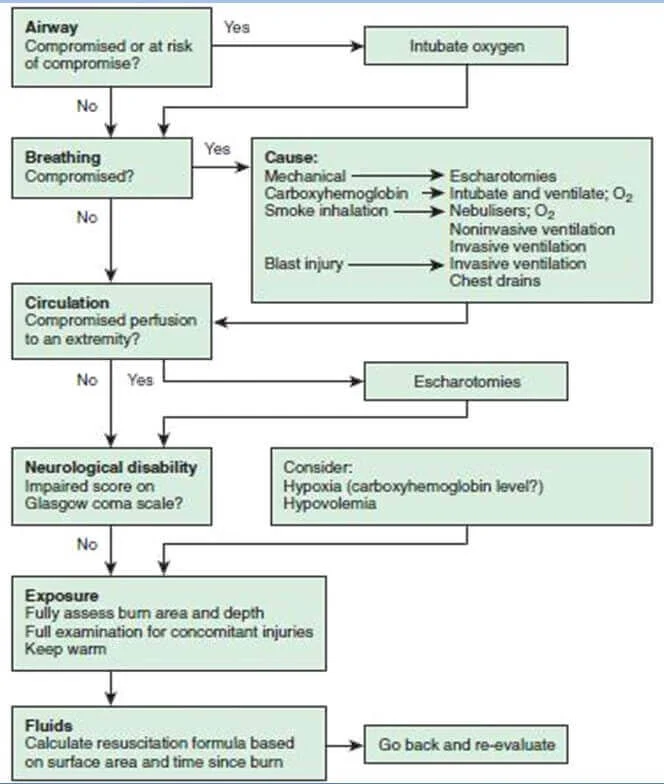
Algorythm for emergency management of Burns
Frequently asked questions in DNB exams
This is a series of solved Pediatrics theory questions. They are not alternatives to thorough textbook reading but can be used for rapid revision at the last moment and also for clinical viva.
Further reading
- Burns - acute management RCH
- Burns - podcast+shownotes
Author

Shailesh Gophane | DCH DNB Pediatrics
Shailesh completed his Pediatric residency from Port Trust Hospital Mumbai after completing DCH from J.J. Hospital, Mumbai
💡 Join the Discussion!
🩺 Help us refine this article — share corrections or additional information below. Let's elevate the accuracy of knowledge together! 💉💬