Juvenile idiopathic arthritis | classification and management guidelines 2021
Introduction
Juvenile Idiopathic Arthritis (JIA) is a most common rheumatologic disease in children that involves joint inflammation and is associated with significant long-term morbidity.
It was previously called Juvenile Rheumatoid Arthritis by the American College of Rheumatology (ACR). Juvenile Chronic Arthritis, is a term coined by (ELAR) European League Against Rheumatism.
Definition
The International League of Associations for Rheumatology (ILAR) defines JIA as
- Arthritis in > 1 joint which is defined as
- Swelling or
- Effusion or
- Presence of 2 or more of the following signs
- Limitation of range of motion,
- Pain or tenderness in motion,
- Increased local temperature.)
- Age of onset, before 16 years
- Duration - Present for at least 6 weeks
- Exclusion of other forms of arthritis in children
Types of JIA
JIA is further classified in sub-categories as
- Systemic-onset JIA
- Oligoarticular JlA
- Polyarthritis (Rheumatoid Factor-negative)
- Polyarthritis (Rheumatoid Factor-positive)
- Psoriatic arthritis
- Enthesitis-related arthritis
- Undifferentiated arthritis
| Category | Definition | Exclusion |
| Systemic onset | Arthritis in 1 joint with, or preceded by a fever of at least 2 wk in duration that is documented to be daily (quotidian) for at least 3 days with 1 of the following. 1. Evanescent (nonfixed) erythematous rash. 2. Generalized lymph node enlargement. 3. Hepatomegaly or splenomegaly or both. 4. Serositis. | a) Psoriasis or a history of psoriasis in the patient or a 1st-degree relative. b) Arthritis in an HLA-B27 - positive boy beginning after the 6 birthday. c) Ankylosing spondylitis, enthesitis-related arthritis, sacroiliitis with inflammatory bowel disease, Reiter syndrome, or acute anterior uveitis, or a history of one of these disorders in an Ist-degree relative. d) Presence of IgM RF on at least 2 occasions at least 3 months apart. |
| Oligoarticular JIA | Arthritis affecting 1-4 joints during the 16 months of disease. Two subcategories are recognized 1. Persistent oligoarthritis affecting ≤ 4 joints throughout the disease course. 2. Extended oligoarthritis affecting > 4 joints after the 1st 6 month of disease | a, b, c, d (above) plus e) Presence of systemic JIA in the patient. |
| Polyarthritis (RF-negative) | Arthritis affecting ≥ 5 joints during the 1st 6 months of disease; a test for RF is negative. | a, b, c,d, e |
| Polyarthritis (RF-positive) | Arthritis affecting ≥5 joints during the 1st 6 months of disease; ≥2 tests for RF at least 3 months apart during the Ist 6 months of disease are positive. | a, b, c, e |
| Psoriatic arthritis | Arthritis and psoriasis, or arthritis and at least 2 of the following 1. Dactylitis. 2. Nail pitting and onycholysis. 3. Psoriasis is an Ist-degree relative | b, c, d, e |
| Enthesitis-related arthritis | Arthritis and enthesitis, or arthritis or enthesitis with at least 2 of the following 1. Presence of or a history of sacroiliac joint tenderness or inflammatory lumbosacral pain or both. 2. Presence of HLA-B27 antigen. 3. The onset of arthritis in a male> 6 yr old. 4. Acute (symptomatic) anterior uveitis. 5. History of ankylosing spondylitis, enthesitis-related arthritis, sacroiliitis with IBD, Reiter syndrome, or acute anterior uveitis in a I st-degree relative. | |
| Undifferentiated arthritis | Arthritis that fulfills criteria in no category or that fits in 2 of the above categories. |
Glossary of terms used in ILAR
What is arthritis?
Swelling within a joint, or limitation in the range of joint movement with joint pain or tenderness, which persists for at least 6 weeks.
Nail pitting
A minimum of 2 pits on one or more nails at any time.
Onycholysis
Detachment of nail from the nail bed.
Enthesitis
Tenderness at the insertion of a tendon, ligament, joint capsule, or fascia to the bone.
Spondyloarthropathy
Inflammation of entheses and joints of the lumbosacral spine.
Serositis
Pericarditis, pleuritis, peritonitis, or a combination of these.
Dactylitis
Swelling of ≥ 1 digit, usually in an asymmetric distribution, that extends
beyond the joint margin.
Inflammatory lumbosacral pain
Lumbosacral pain at rest with morning stiffness, which improves on movement.
Etiology & Pathogenesis
|
|
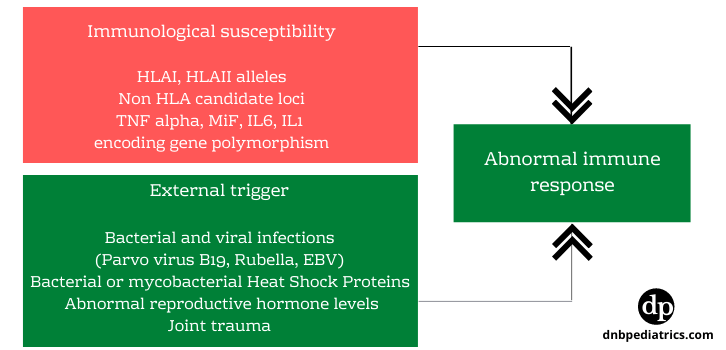
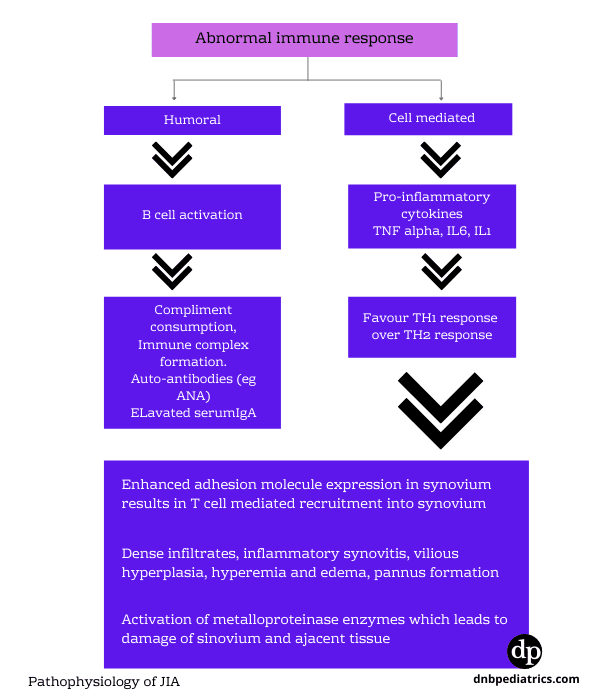
| Image 1. Etiopathogenesis |
A. All forms of JIA other than systemic-onset JIA, are disorders of adaptive immunity autoimmune disorders.
What is adaptive immunity - autoimmune disorder?
Lymphocytes (TH, cells) play a major role in pathogenesis. Self-antigens are considered foreign and attacked.
B. Systemic onset JIA is a disorder of innate immunity, an autoinflammatory disorder.
What is an Innate immunity - autoinflammatory disorder?
Normally innate immunity is the first line of defense. It is a nonspecific response we naturally possess to fight foreign antigens. Neutrophils, monocytes & macrophages play a major role in the pathogenesis of auto-inflammatory disorders.
The balance between pro-inflammatory cytokines such as TNF-a, IL-I, IL-6, IL-8, and anti-inflammatory cytokines such as IL-4, IL-10, IL I receptor antagonists determines the degree of joint damage and severity of arthritis.
General Clinical features in JIA
- Involved joints are often swollen, warm to touch, and painful on movement or palpation with reduced range of motion but usually are not erythematous.
- Morning stiffness with a limp or gelling after inactivity.
- Easy fatigability and poor sleep quality may be associated.
- Arthritis in large joints, especially knees, initially accelerates linear growth, causing the affected limb to be longer and resulting in a discrepancy in limb lengths.
- Continued inflammation stimulates rapid and premature closure of the growth plate, resulting in shortened bones.
Clinical manifestations in systemic-onset JIA
- Systemic JIA is characterized by arthritis, fever, and prominent visceral involvement, including hepatosplenomegaly, lymphadenopathy, and serositis (pericarditis).
- Quotidian fever. The fever is often present in the evening.
- Characteristic faint, erythematous, macular rash. The evanescent salmon-colored lesions are linear or circular and are most commonly distributed over the trunk and proximal extremities. It is nonpruritic and migratory with lesions lasting <I hr. Koebner phenomenon is often present. Heat, such as a warm bath towel, can evoke rash.
- Arthritis is classically polyarticular, may be very destructive, and includes the hip, cervical spine, and TMJ.
Clinical manifestations of Oligoarticular JIA
- Oligoarthritis involves large joints of the lower extremities, such as the knees and ankles. Often only a single joint is involved.
- Involvement of the hip almost never occurs and if present suggests a spondyloarthropathy or non-rheumatologic cause.
- The presence of a positive antinuclear antibody (ANA) test result confers increased risk for asymptomatic anterior uveitis, requiring periodic slit-lamp examination.
Clinical manifestations of Polyarticular JIA
- RF positive polyarticular disease resembles the characteristic symmetric presentation of adult rheumatoid arthritis.
- Rheumatoid nodules on the extensor surfaces of the elbows and over the Achilles tendons are associated with a more severe course and almost exclusively occur in RF-positive individuals.
- Chronic Temporomandibular joint (TMJ) disease results in micrognathia.
- Cervical spine involvement, manifesting as decreased neck extension, occurs with a risk of atlantoaxial subluxation and neurologic sequelae.
- Hip disease may be subtle, with findings of a decreased or painful range of motion on the exam.
Demographic features of JIA
| Category | Peak age of onset | Male to female ratio | Arthritis pattern | Extraarticular features |
| Systemic onset | 2.4Yrs | 1:1 | Poly articular, often affecting knees, wrists and ankles, also fingers, neck and hips | Daily fever, evanescent rash, pericarditis, pleuritis. Oligo arthritis |
| Oligoarticular JIA | <6Yr | 4:1 | Knees ++ ankles, fingers + | Uveitis in 30% of cases |
| Polyarthritis (RF-negative) | 6-7 Yrs | 3:1 | Symmetric or asymmetric, small and large joints, cervical spine, TMJ involvement | Uveitis in 10% of cases |
| Polyarthritis (RF-positive) | 9-12 Yrs | 9:1 | Aggressive, symmetric polyarthritis | Rheumatoid nodules in 10% Low-grade fever |
| Psoriatic arthritis | 7-10 Yrs | 2:1 | Asymmetric arthritis of small or medium-sized joints | Uveitis in 10%, Psoriasis in 50% |
| Enthesitis-related arthritis | 9-12Yrs | 1-7 | Predominantly lower limb joints affected, sometimes axial skeleton but less than in adults. | Acute anterior uveitis, association with reactive arthritis and IBD |
Laboratory findings & investigations
Hematology
- Hemogram showing anemia of chronic disease with elevated WBC and platelet counts and microcytic anemia on PS
- With low WBC count and low platelet count, keep suspicion about Macrophage Activation Syndrome (MAS)
- Elevated ESR and C-reactive protein (CRP) can be seen
Serology
Elevated ANA titers - Can be seen in 40-85% of children with oligoarticular or polyarticular JIA. These are rarely seen in SoJIA. ANA can be associated with an increased risk of chronic uveitis in JIA.
Rheumatic Factor - 5-10% of patients with polyarticular JIA are seropositive for RF.
Anti-cyclic citrullinated peptide (CCP) antibody - Like RF, it is also a marker of more aggressive disease.
HLA-B27 - is positive in enthesitis-related form.
Radiology Investigations
Xray
Continued active disease may lead to early radiographic changes of arthritis such as
- Soft tissue swelling
- Periarticular osteoporosis and
- Periosteal new-bone apposition
- Subchondral erosions
- Loss of cartilage
- Varying degrees of bony destruction and, around affected joints.
- Fusion.
MRI
MR is more sensitive than X-rays to early changes. It is also the most sensitive
radiologic indicator of disease activity. It can depict
- Synovial hypertrophy,
- Define soft tissue swelling,
- Demonstrate excellent detail of articular cartilage and
- Anatomy of overall joint integrity.
Investigations for extra-articular manifestations
- Cardiac examination and ECHO for pericarditis
- Ocular examination for Uveitis
- Chest examination for pleuritis
Management
Children with JIA should be managed with a multidisciplinary approach and need individualized treatment plans. The management is tailored according to
Disease subtype
Severity
Presence of poor prognostic indicators, and
Response to medications.
Management involves one or all of the following areas
- Pharmacologic management
- Psychosocial factors, including counseling for patients and parents
- School performance, such as academic counseling, school-life adjustments, and physical education adjustments.
- Nutrition, particularly to address anemia and generalized osteoporosis
- Physical therapy, to relieve pain and address range of motion, muscle strengthening, activities of daily living, and conditioning exercises.
- Occupational therapy, including joint protection, a program to relieve pain, range of motion, and attention to activities of daily living
Pharmacologic management
The primary goals of medical therapy are
- To eliminate active disease
- To normalize joint function
- To preserve normal growth
- To prevent long-term joint damage
Commonly used drugs in the present-day treatment of JIA
Anti-inflammatory drugs
NSAIDs
- Ibuprofen
- Naproxen
- Indomethacin
- Meloxicam
Steroids
- Intraarticular triamcinolone
- Oral prednisolone
- Methyl prednisolone
- Topical ocular preparations prednisolone
Disease-Modifying Anti-rheumatic Drugs (DMARD)
Conventional DMARD (csDMARD)
- Methotrexate
- Sulfasalazine
- Leflunomide
- Cyclosporin
Biological DMARD (bDMARD)
- Adalimumab
- Etanercept
- lnfliximab
- Abatacept
- Toclizumab
- Rituximab
- Anakinra
- Canakinumab
- Rilonacept
Non-steroidal anti-inflammatory drugs (NSAIDs) in JIA
Historically NSAIDs have been the mainstay of treatment for JIA in children however the modern approach is to introduce disease-modifying agents DMARDs
early in the course of the disease.
NSAIDs are frequently used as adjunctive therapy to more definitive therapies for symptom control. NSAIDs control the symptoms without altering the natural history of the
disease.
In general, NSAIDs should only be considered as monotherapy for initial therapy in less severe forms. If control is not achieved within 4 to 6 weeks additional therapy must be considered.
One of the main actions of NSAIDs is the inhibition of cyclooxygenase (COX) which decreases the production of prostaglandins resulting in analgesia.
Side effects of NSAIDs
- Bleeding by inhibition of platelet function
- Gastrointestinal (GI) toxicity
- Pseudoporphyria - Naproxen
- Headache, mood change, and decreased school performance
- Liver toxicity
- Renal toxicity
ACR Recommendations for monitoring of NSAIDs in JIA patients
What to monitor?
- Complete blood cell count,
- Liver enzymes,
- Serum creatinine
When to monitor?
- Prior to or soon after initiation of routine use
- Repeat twice yearly for chronic daily use
- Repeat one yearly for routine use (4 days per week)
Corticosteroids in the treatment of JIA
Mechanism of action
In physiologic low-doses
Binds to cytosolic receptors >> translocate as a complex, to the nucleus >> the complex binds to DNA >> induces mRNA transcription of some genes encoding for anti-inflammatory
proteins and decreases the transcription of genes encoding pro inflammatory proteins.
At higher doses
Rapid, non-receptor-mediated events occur, causing apoptosis (programmed cell death) of lymphocytes and other inflammatory cells.
Intra-articular corticosteroids (IAGc)
The use of intra-articular Triamcinolone hexacetonide (THA), 1 mg/kg in large joints such as the knee and 0. 5 mg/kg in smaller joints such as the ankle, has been found to be superior to Triamcinolone acetonide.
- Early treatment is associated with better outcomes.
- Difficult-to-reach joints such as the hip, sacroiliac (SI) joint, temporomandibular joint (TMJ), and the subtalar joint may be injected using ultrasound or fluoroscopy.
- The use of IASs for active arthritis has been recommended by the ACR guidelines regardless of concurrent therapy, JIA subtype, disease activity, prognostic features, or joint contracture.
Oral corticosteroids
- Oral glucocorticoids are usually not recommended.
- Oral glucocorticoids are given to quickly alleviate severe symptoms when an IAGc is not available or feasible, or prior to the onset of action of disease-modifying antirheumatic drugs (DMARDs)
- Treatment should be limited to the lowest effective dose for the shortest duration possible.
Systemic corticosteroids
ACR does not recommend systemic corticosteroid use, except
- In systemic juvenile idiopathic arthritis (sJIA) for severe systemic features and
- In polyarticular JIA, in order to bridge constitutional features of pain and fatigue while waiting for DMARDs or biologic therapies to reach their therapeutic effect. (Bridge therapy)
Toxicity
- Obesity,
- short stature,
- hypertension,
- osteoporosis,
- cataracts,
- mood changes,
- diabetes mellitus,
- avascular necrosis, and
- susceptibility to infection.
Conventional synthetic DMARDs (csDMARD)
Conventional synthetic DMARDs are strongly recommended if there is an inadequate response to scheduled NSAIDs and/or IAGCs for active oligoarthritis.
Methotrexate is conditionally recommended as a preferred agent over leflunomide, sulfasalazine, or hydroxychloroquine (in that order).
Methotrexate
- Methotrexate is the most commonly used DMARD in JIA.
- Starting methotrexate early leads to a better response.
- Maximum dose of 0.6 mg/kg once weekly (equivalent to 15 mg/m/week, maximal 25 mg/week) of parenteral MTX.
- Daily folate supplementation at I mg/day along with methotrexate.
Mechanism of action
The current and the most possible mechanism is that methotrexate increases adenosine levels and on the engagement of adenosine with its extracellular receptors an intracellular cascade is activated promoting an overall anti-inflammatory state.
Methotrexate also inhibits dihydrofolate reductase, preventing the reduction of dihydrobiopterin (BH2) to tetrahydrobiopterin (BH4), which leads to nitric oxide synthase uncoupling and increased sensitivity of T cells to apoptosis, thus reducing immune responses.
Side effects
- Nausea, vomiting, oral ulcerations,
- Hepatitis,
- Blood dyscrasias and
- Immunosuppression.
ACR Recommendations for monitoring of Methotrexate in JIA patients
What to monitor?
Complete blood cell count, liver enzymes, serum creatinine
When to monitor?
- Prior to initiation
- 1 month after initiation
- 1-2 months after an increase in dose
- Every 3-4 months if prior results are normal and the dose is stable.
Sulfasalazine
- Sulfasalazine and its metabolites are weak inhibitors of cyclooxygenase (both COX-I and COX-2).
- Sulfasalazine inhibits folate metabolizing enzymes such as DHFR.
- Sulfasalazine is efficacious, particularly in Enthesitis-Related Arthritis.
- It is contraindicated for use in Systemic Arthritis, at least during the acute phase of the disease, because of good evidence of increased toxicity in this situation
Adverse effects
- GI upset,
- Allergic reaction,
- Pancytopenia,
- Renal and hepatic toxicity.
Biologic DMARDs (bDMARD)
Biologic DMARDs are strongly recommended if there is an inadequate response to or intolerance of NSAIDs and/or IAGCs and at least 1 conventional synthetic DMARD for active oligoarthritis. There is no preferred bDMARD.
The tumor necrosis factor inhibitors (TNFi) are the most commonly used bDMARDs in children.
TNF - alpha inhibitors
- Adalimumab,
- Etanercept,
- Infliximab
Other biologicals
- Abatacept
- Canakinumab
- Rilonacept
Mechanism of action
- Adalimumab - act by inhibiting pro-inflammatory cytokine TNF-a
- Abatacept (CTLA4-Ig) - T cell co-stimulatory inhibitor
- Canakinumab - Human monoclonal antibody targeted at interleukin-I 3
- Rilonacept - Interleukin-I inhibition
- Anakinra - Interleukin-I receptor antagonist
- Tocilizumab - Humanized monoclonal antibody against the IL-6 receptor
- Rituximab - chimeric monoclonal antibody against CD-20
Adverse effects
- Serious infections,
- Demyelinating processes, optic neuritis,
- Injection site reactions or infusion reactions,
- Development of autoimmune conditions and reactivation of tuberculosis.
ACR Recommendations for monitoring of TNF -a inhibitors in JIA
- Complete blood cell count, liver enzymes, serum creatinine prior to initiation and then every 3-6 months
- Tuberculosis screening - prior to initiation and then, once yearly
2019 and 2021 ACR recommendations for pharmacotherapy of Juvenile Idiopathic Arthritis
American College of Rheumatology (ACR) revised guidelines for Systemic Juvenile Idiopathic Arthritis, Oligoarthritis, Temporomandibular Joint Arthritis in 2021 and revised guidelines for the Treatment of Juvenile Idiopathic Arthritis subtypes Non- Systemic Polyarthritis, Sacroiliitis, and Enthesitis in 2019
Treatment algorithm for systemic juvenile idiopathic arthritis 2021 Update
The management protocol is divided based on the presence or absence of MAS

|
| Image 2. Management of systemic JIA |
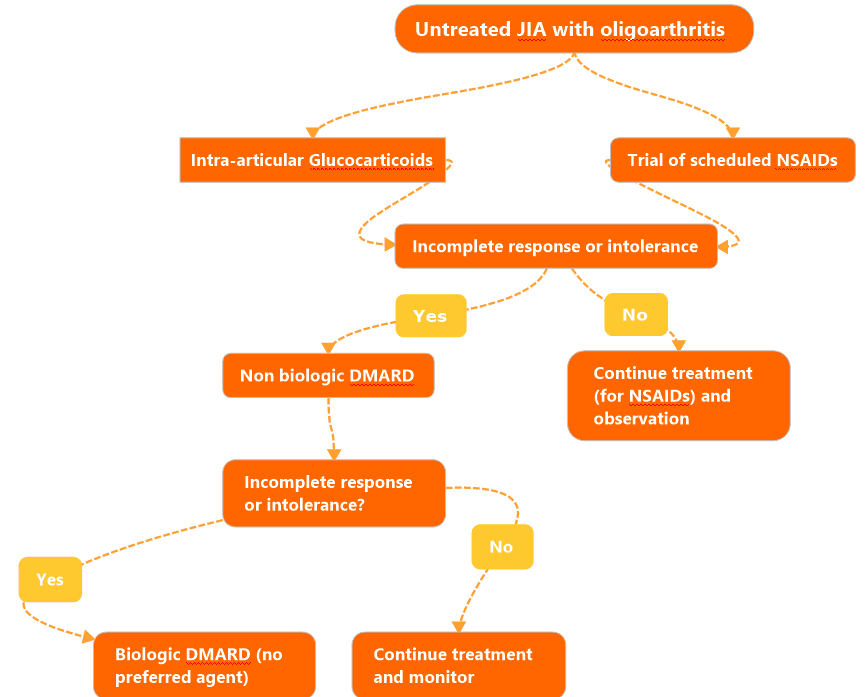
Treatment algorithm for oligoarticular JIA 2021 update.
|
| Image 3. Management of oligoarticular JIA |
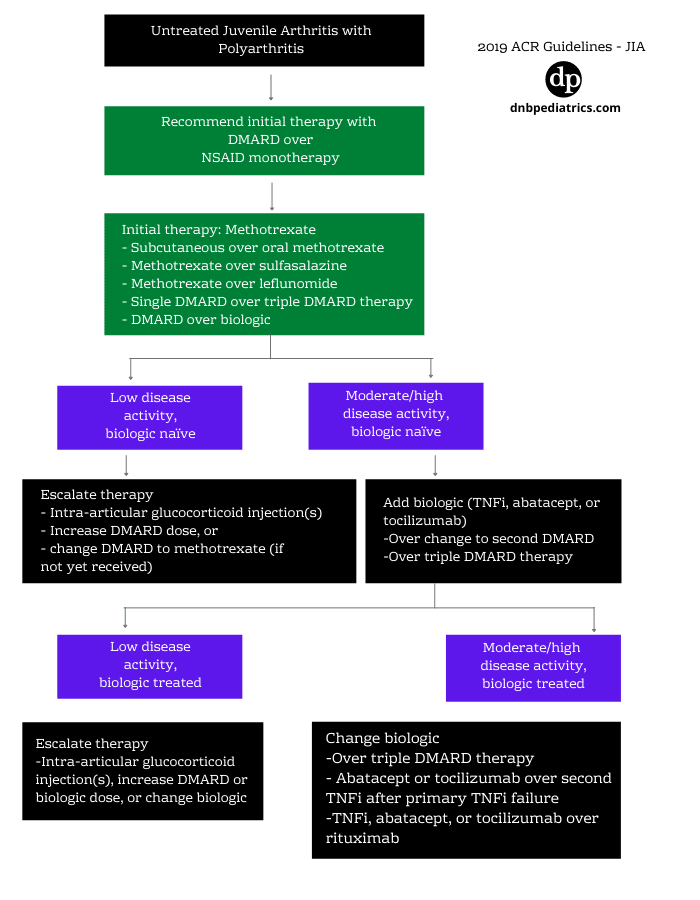
Treatment algorithm for Polyarticular JIA 2019 update.
|
| Management of polyarticular JIA |
Treatment guidance for Enthesitis associated JIA 2019 update
- NSAID treatment is strongly recommended over no treatment with an NSAID.
- Use of TNFi is conditionally recommended over methotrexate or sulfasalazine in active enthesitis despite treatment with NSAIDs.
- Bridging therapy with a limited course of oral glucocorticoids (<3 months) during initiation or escalation of therapy.
- Bridging therapy may be more useful in cases with high disease activity, limited mobility, and/or significant symptoms.
References
- 2021 American College of Rheumatology Guideline for the Treatment of Juvenile Idiopathic Arthritis: Therapeutic Approaches for Oligoarthritis, Temporomandibular Joint Arthritis, and Systemic Juvenile Idiopathic Arthritis.
- 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Treatment of Juvenile Idiopathic Arthritis: Therapeutic Approaches for Non- Systemic Polyarthritis, Sacroiliitis, and Enthesitis
- Prakken B, Albani S, Martini A. Juvenile idiopathic arthritis. Lancet. 2011;377(9783):2138-2149.
- Petty RE, Southwood TR, Manners P, et al. International League of Associations for Rheumatology. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31:390-392.
Author

C. Naveen Kumar| MD Pediatric
Naveen is MD in pediatrics and completed his residency from SV medical college, Titupati.
Update

Ajay Agade | DNB(Pediatrics), FNB(Pediatric Intensive Care), Fellowship in Pediatric pulmonology and LTV
Ajay is a Paediatric Intensivist, currently working in Pediatric Pulmonology & LTV at Great Ormond Street Hospital NHS, London
💡 Join the Discussion!
🩺 Help us refine this article — share corrections or additional information below. Let's elevate the accuracy of knowledge together! 💉💬